Compartment pressure checks should be reserved for patients who are difficult to examine, such as sedated patients or those with equivocal examination findings. Adhesive capsulitis can be protracted, with the mean duration of symptoms 30 months. Assessing the anteroinferior capsule: A loss of passive external rotation in abduction suggests contracture of the anteroinferior capsule. The umbilicus is a weaker area of the abdominal wall through which various inflammatory processes can drain and give rise to acquired fistulas. Abscesses underlying the abdominal wall are accompanied by signs of local peritoneal irritation. Arthroscopic view of the subscapularis insertion of a right shoulder from the posterior portal using a 30-degree arthroscope with the arm in 30 degrees of abduction and neutral rotation (B) and in internal rotation (C). It should be noted that after abdominal operations, especially laparoscopic surgery, air may be present within the abdominal wall during the early post-operative period. Patients with pelvic fractures may become hemodynamically unstable, and close monitoring of blood pressure and fluid requirements is needed. This gives rise to narrowing and occlusion of the vessel with consequent distal ischaemia. Lesions with considerable symphyseal comminution unreceptive to anterior plating may be managed to union with external fixation, provided the posterior tension band remains functionally intact. The standard arthroscopic setup and equipment includes the 4-mm 30-degree arthroscope. The intra-articular microenvironment must be protective of this complicated interaction of the implantated chondrocytes and the stimulutory aspects of the rehabilitation, such as early motion to allow for the remodeling and maturation of these chondrocytes into a hyaline-like cartilage phenotype. An attempt is made to trim all of the acetabulum with abnormal articular cartilage to a residual lateral center edge angle of 25 to 30 degrees, taking more or less according to the preoperative center edge angles. Arthroscopic synovectomy in rheumatoid and psoriatic knee joint synovitis: long-term outcome. After all the tubal products have been either extruded or resorbed, the hormone levels return to baseline and the vaginal bleeding stops. During evaluation, pay attention to the position of the patient, their facial expression and their overall comfort level. Palpation of insertion of conjoint tendon: tenderness may increase, and a bulge may be felt by having the patient perform a Valsalva maneuver. Skeletally immature children may still be considered for some form of intramedullary treatment after considering remaining growth, type of fracture, and benefits over other methods of treatment. The femoral nerve may be difficult to examine secondary to pain associated with the fracture. The internal opening may be felt digitally as an indurated nodule or pit, or may be seen at proctoscopy, aided if necessary by gentle downward retraction of the dentate line, which may expose openings concealed by prominent anal valves. Uncomplicated acute appendicitis is not associated with symptoms of bowel obstruction. Diagnostic accuracy of clinical tests for the different degrees of subacromial impingement. Perforate the posterior tibial cortex by hand with the guide pins or reamers in a controlled fashion under direct arthroscopic visualization to avoid neurovascular injury. Biceps long head abnormalities can include: Hyperemia, seen in patients with adhesive capsulitis or in biceps instability Overt subluxation: Most commonly subluxation is inferior due to injury to its inferior restraints, composed of the upper subscapularis tendon, or bicipital sling, composed of Preoperative Planning Clinical evaluation to determine the contribution of the biceps tendon to patient symptoms is an important component of decision making and helps when encountering biceps pathology. Nonoperative management may be best employed in the already degenerative hip with joint space narrowing prior to total hip arthroplasty, and consists of activity modification, core trunk strengthening exercises, and occasional intra-articular corticosteroid or hyaluronic acid injections. Occasionally internal rotatory instability is sufficient to warrant surgical stabilization (external or internal fixation). Predistention Epinephrine for vasoconstriction Appropriate pump pressure the surgeon should work expeditiously. It is important to ensure that the patient understands that full-thickness lesions have little spontaneous healing capacity and that further degeneration is likely. On physical examination, there may be a tender flank mass secondary to a urinoma, signs of peritionitis or urine leakage from the wound or vagina. Preparation and draping of the leg using a flat-top table without traction should include posterior sections of the buttocks. Examination is usually limited to direct palpation of the groin and the base of the labium majus. The lateral collateral ligament originates on the lateral epicondyle of the femur and attaches to the fibular head.
Syndromes
Chisel inserted after femoral head and neck and trochanteric block were secured with lag screws. Vessels from the perimeniscal capillary plexus proliferate throughout this fibrin scaffold and are accompanied by the proliferations of differentiated mesenchymal cells. Ruptures usually occur transversely through the tendon at a pathologic area approximately 2 cm proximal to the superior pole of the patella, and then progress obliquely into the medial and lateral retinacula based on the amount and duration of force. This relaxes the iliotibial band, eliminating the snapping, without creating any suture repair lines that would necessitate prolonged convalescence. With the patient supine, a compression bandage is applied to the leg tightly enough to occlude the superficial venous system. Landmarks for posterior pin placement include the anterior superior iliac spine, posterior superior iliac spine, and dorsal axis of the femur. Hip-to-ankle films may be helpful in chronic cases to evaluate for varus malalignment. If no objective cause can be identified, it is termed idiopathic urge incontinence, whereas neurogenic detrusor incontinence occurs secondary to neurological disease, for example multiple sclerosis, motor neurone lesions and peripheral nerve lesions following pelvic surgery. Urothelial cell carcinomas are associated with cigarette smoking and occupational chemical carcinogens. Further research is required to develop the optimal rehabilitation programs after the various procedures that have been discussed. Closure of Rotator Interval Plication Stitches If the posterior labrum is intact but posterior laxity remains, plication stitches can be placed to better balance the anterior and posterior tension on the inferior glenohumeral ligament. Core decompression will not improve symptoms once collapse has occurred, because the joint surface then is irregular and essentially arthritic. The suprascapular nerve, artery, and vein are allowed to fall back into a relaxed position. Additional concerns when treating pelvic ring trauma include injury to the lumbosacral and coccygeal nerves and male urethra. Special tests have been developed to aid in diagnosis: the Neer impingement test (forward elevation in internal rotation) and the Hawkins impingement test (elevation to 90 degrees, cross-body adduction and internal rotation) were designed to elicit symptoms by impinging the rotator cuff on the undersurface of the acromion and coracoacromial ligament. Despite lack of donor cell viability, allograft survival and outcome of meniscal transplant have not been affected. If the patient is obese, it is essential to have an assistant retract the left buttock and thigh to expose the anus. Surgery, therefore is indicated in patients who cannot tolerate activity restriction. The tibial fracture is distracted and reduced using a mechanical distraction device with proximal and distal half-pins. Approach Adequate fixation and accordingly proper pin placement are the principal requirements for restoring pelvic stability when applying an external fixator. This is frequently associated with a prodrome of gastroenteritis when lymphoid aggregates with the bowel wall hypertrophy and serves as lead points for the intussusception. Psoas tenotomy and heterotopic ossification after Charnley low-friction arthroplasty. We have found that patients may have a history of siblings, parents, and grandparents with hip pain or osteoarthritis of the hip, and patients may have milder or similar symptoms in the contralateral hip. Throwing athletes are prone to shoulder dysfunction due to chronic fatigue and weakening of the posterior shoulder musculature that over time leads to maladaptive contracture of the posteroinferior glenohumeral joint capsule. Pinch of capsular and ligamentous tissue with shuttling instrument coming from posterior portal to place at inferior aspect. Anterior capsulectomy is performed with arthroscope posterior and instruments anterior. If the hip is irreducible, or there is an associated femoral neck fracture, emergent open reduction and internal fixation are required. Double-Bundle Tunnel Preparation A long drill-tip guidewire is placed through the inferolateral portal with the knee positioned at 90 degrees, viewing the pin placement from an inferomedial portal.
The physical examination should identify disease-specific signs to assess for the likelihood of each possible diagnosis. Proximity of iliosacral screws to neurovascular structures after internal fixation. The muscle forces are shown on the distal femur, as is the femoral artery and vein entering the canal of Hunter (arrow). The guide pin is removed and the solid end of the Nitinol wire loop is passed antegrade through the cannulated reamer. Trichomonas vaginalis infection causes a profuse, watery, pale yellow, sometimes frothy discharge with intense pruritis. Comparison of surgical repair of the cruciate ligament versus nonsurgical treatment in patients with traumatic knee dislocations. Discoid menisci are abnormal in terms of both mobility and tissue bulk, making them vulnerable to compression and rotary stress. Arthroscopy of the elbow: anatomy, portal sites, and a description of the proximal lateral portal. No suction is used while the burr is operating to prevent inadvertent injury to labral tissue. Meniscal repair compared with meniscectomy for bucket-handle medial meniscal tears in anterior cruciate ligament-reconstructed knees. A patient without locking typically gives a history of several episodes of trouble referable to the knee, often resulting in effusion and a brief period of disability but no definite locking. Scar formation from any surgery or trauma can engulf a peripheral nerve and compress it; symptomatic relief can then be accomplished through surgical decompression of the peripheral nerve. An omphalocele is characterized by extruded abdominal contents covered by a sac composed of amnion. Generally 5 mm of acetabulum is trimmed with more removed based on the extent of chondral damage taking care not to create a dysplastic acetabulum based on preoperative center edge angles. The extremity should be draped free from the anterior superior iliac spine to the ankle. The knot is placed on the periosteum side, not the cartilage rim, to prevent shearing. With extension of the hip, the iliospoas shifts medial to the center of the femoral head. Colicky abdominal pain (lead colic) and constipation may simulate an acute abdomen. Arthroscopic decompression and physiotherapy have similar effectiveness for subacromial impingement. In rheumatoid arthritis, the cervical spine is commonly involved and must be evaluated before surgical intervention. Alternatively, the surgeon may make multiple passes through the biceps tendon (using a locking stitch of nonabsorbable suture such as FiberWire) and then use a knotless-type anchor (such as the Arthrex "push-lock" or "swivel-lock") to perform a secure tenodesis in a percutaneous fashion over a previously placed small-diameter cannula. After injection of the cells is completed, the needle is withdrawn, and the small opening for the angiocatheter is then sutured with 6. Results of intertrochanteric femur fractures treated with a 135-degree sliding screw with a twohole side plate. Nonetheless, this system is widely employed in the femur for descriptive purposes. The level of compressive load affects conclusions from statistical analyses to determine whether a lateral meniscal autograft restores tibial contact pressure to normal: a study in human cadaveric knees. A suction drain is typically used for 24 hours postoperatively to minimize hemarthrosis. A positive psoas sign (an exacerbation of pain on passive hyperextension of the right thigh with the patient lying on left side) may be present. The normal Insall-Salvati ratio (height of the patella over the distal from the inferior pole to the tibial tubercle) is about 1.
Various ablation devices can be used to contour tears; however, care must be taken not to damage adjacent articular cartilage. A comparison of results in acute and chronic anterior cruciate ligament ruptures of arthroscopically assisted autogenous patellar tendon reconstruction. After the capsulotomy is performed, blunt retractors are placed around the femoral neck to expose the femoral head and neck. Early passive motion has historically been recommended after open rotator cuff repair. They are composed of dense, tightly woven collagen fibers arranged in a pattern providing great elasticity and ability to withstand compression. Pyoderma gangrenosum appears as ulcerated skin lesions and may occur independent of disease activity. In the younger woman, this is usually neurological in origin and may represent the onset of a more widespread neurological disease such as multiple sclerosis. The seminal vesicles and vasa, neither of which is palpable in the normal individual, lie cranial to the prostate. Intraoperative lateral fluoroscopic view showing position of the temporary stabilization pin and the guidewire. The role of arthroscopy in the treatment of postoperative fibroarthrosis of the knee joint. Areas requiring particular attention in disabled throwers include superior labrum and biceps anchor, rotator cuff insertion, posterior capsule and recess, and anteroinferior labrum and capsule. Typical setup for semi-extended nailing with a small bolster for limited knee flexion and easy access to the limb for reduction and imaging. The pathophysiological mechanism responsible for the most severe complication of incarcerated hernias is: a Gastrointestinal bleeding b Ischaemia c Intestinal obstruction d Pain e Urinary difficulty Answer b Ischaemia. The superior lumbar hernia originates through the triangle of Grynfeltt, which is bounded by the 12th rib superiorly, the posterior border of the internal oblique muscle inferiorly and the erector spinae and quadratus lumborum muscles medially. The prevalence of full-thickness tearing of the rotator cuff ranges from 7% to 40% across multiple studies. The suture should be placed 10 to 20 mm distal to the exposed proximal portion, depending on how much diseased tendon is present, how much was resected intraoperatively, and the intended location of the tenodesis. Recurrent instability affecting daily activities despite formal physical therapy generally requires surgical treatment. On average, 38% of multiligament knee injuries require at least one surgical intervention to regain motion. A longitudinal incision starting from the ischial tuberosity, over the posterior thigh, is used in chronic cases requiring significant mobilization or fractional lengthening of the hamstrings or sciatic neurolysis. In their undiseased state they act as physiologic check reins at extreme ranges of motion. Starting 12 weeks after microfracture, the exercise program is the same as that used for femorotibial lesions. However, the posterolateral portal is important for routine inspection of the posterior recesses as well as access for posteriorly based lesions and the acetabular fossa. This helps to protect the soft tissues in this area from damage and reduces fluid extravasation into the surrounding soft tissues. Such local skin changes must be differentiated from skin changes caused by external factors. Line Z crosses the anterior aspect of the lateral condyle (point A) and line X (point C). Articular cartilage is a smooth, viscoelastic, hypocellular structure with a low coefficient of friction (estimated to be 20% of the friction seen with ice on ice) and the ability to withstand significant recurring compressive loads. On examination, the fluid within the hydrocele transilluminates and can be compressed and drained back into the abdomen. These hernias frequently present as intestinal obstruction and may be difficult to diagnose. A clot will form, which is blotted dry and then inserted using an arthroscopic grasper to the repair site.
A Cobb elevator is used to create a plane submuscularly up the lateral shaft of the femur for placement of the plate. If a significant portion of the peripheral rim can be retained by subtotal meniscal excision, the long-term result is improved. Using a combination of electrocautery, motorized shavers, arthroscopic knives, or heavy scissors, the suprapatellar pouch is reconstituted by performing aggressive releases. Chapter 55 Common Peroneal and Lateral Femoral Cutaneous Nerve Injuries Ivica Ducic and Jeffrey M. This is often seen in cases of unrecognized lateral wall fractures (either iatrogenically induced by implant placement or unrecognized from the original trauma). For a mattress suture, the process of capsular plication with a suture-passing device and subsequent suture shuttling is repeated so that both limbs of the suture exit the tissue on the tissue side. If the pin is not centered in the head on both views, it must be removed and adjusted. The narrow and curved profile of the crest does not allow parallel pin insertion and on occasion accommodates no more than two pins. On physical examination, urethral diverticula can be felt as a mass behind the urethral meatus, which on compression may elicit discomfort and/or a purulent discharge. This has been described as the "killer turn" or "killer curve," which may cause graft abrasion and subsequent failure. We prefer bilateral foot traction with knees in extension with the legs scissored, although attachment to the fracture table via skeletal traction through the distal femur or proximal tibia is used if there are other injuries about the knee, leg, or foot. After the reamer has been inserted about 20 mm, its trajectory is confirmed with a lateral C-arm view. A blunt obturator or switching stick can be used to bluntly dissect the deep capsule from the more superficial anterior subscapularis (subscap) tendon. The condition usually presents in middle age with nonspecific symptoms, including poorly localized back pain, fever, anorexia, weight loss and malaise. The highest measurement is compared to the diastolic blood pressure and interpreted accordingly. Evaluation of Patients with Abdominal Pain 555 production from a gastrin-secreting tumour, usually located within the pancreatic head. Imaging demonstrates dilatation of the colon to greater than 6 cm and variable degrees of bowel wall thickening. The presence or absence of these fibers must be confirmed to ensure a complete tenotomy is accomplished. Maintaining the same angle, the surgeon replaces the hemostat with a blunt trocar in an operative cannula. Occlusion of the apocrine gland ducts leads to bacterial proliferation within the glands, with rupture and the spread of infection to adjacent glands. Failure of external rotation to eliminate the sulcus sign may indicate multidirectional instability or global laxity. The arterial insufficiency may need to be addressed first in order to allow for the use of compression therapy. A rapid increase in intraluminal pressure in the stomach and oesophagus may produce barotrauma of the distal oesophagus. The tip of the anterolateral aspect of the acromion is palpated with the resector to confirm the correct subacromial orientation. With proper diagnosis, the surgical results for snapping of the iliopsoas tendon and the iliotibial band are highly predictable and finite in terms of resolution of the snapping. Other indications include the stabilization of closed fractures with high-grade soft tissue injury or compartment syndrome. When a screw that blocks the way is encountered, simply push the reamer head past the screw without reaming. The psoas major originates from the lumbar transverse processes and the sides of the vertebral bodies and intervertebral discs from T12 to L5; the iliacus originates from the superior two thirds of the iliac fossa, the sacral ala, and the anterior sacroiliac ligaments.
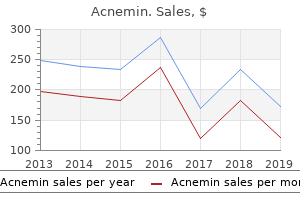
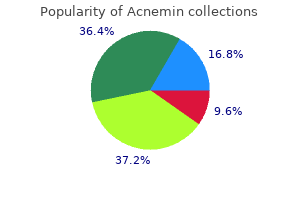
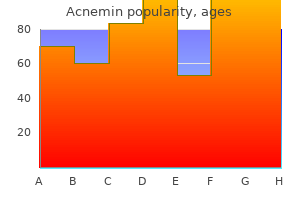
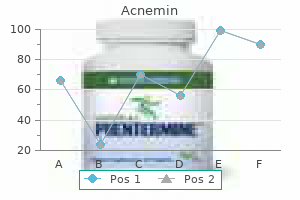
Vitamin B17 (Apricot Kernel). Acnemin.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97133
Recognition and treatment of refractory posterior capsular contracture of the shoulder. In such cases, a misdiagnosis of the pathology may occur unless an incarcerated hernia is considered in the differential diagnosis and a thorough examination is performed. The patient is started on a passive stretching program that includes passive external rotation with a cane up to 45 degrees and overhead stretches with a rope and pulley. Accurate pin placement within the curved iliac crest mandates a nonparallel converging pin pattern. Patient compliance is an issue owing to the minimally invasive nature of the surgery. Acute Pyelonephritis Acute pyelonephritis is defined as inflammation of the renal parenchyma and renal pelvis. Extrinsic contracture: "the column procedure"-lateral and medial capsular releases. The ureter then courses downwards and backwards to the level of the ischial spine before turning forwards and medially to enter the posterior wall of the bladder. The surgeon must assess for valgus instability when considering valgus extension overload. In principle, less dissection and soft tissue retraction, as well as optimal implant placement, should be possible using more direct approaches. Above the dentate line, the epithelium is relatively insensitive, although an appreciation of stretch can be elicited. Approach the first arthroscopic portal is anterior except when the entire procedure is accomplished through posterior portals. We prefer to have the anesthesiologist provide sedation in conjunction with a local anesthetic administered by the surgeon. Early sheeting (circumferential external compression) may offer an initial beneficial hemodynamic response. Intra-articular injury, if present, is typically simple and without comminution or impaction. Arthroscopy reveals a traumatic detachment of the anterior labrum (indicated by the probe). Lateral compression injuries, depending on severity, may result in internal collapse of the pelvis. An assistant should hold cannulas in the joint once they are passed through the capsule, particularly during suture passage and knot tying, or the cannulas will back out and allow distention of superficial tissues. Anatomic studies suggest three guidelines for neurovascular safety: Portal placement is safer when the elbow is flexed 90 degrees than when it is in extension. After 4 weeks, the athlete is prepared to return to functional activities with more strengthening, endurance, and flexibility. The degree of flexion at which this crepitus or pain occurs is important in localizing the location of the lesion, bearing in mind that the articulation surface of the patella moves proximally as the knee is flexed. If there is compression and narrowing of the vein at the costoclavicular junction, patients should undergo thoracic outlet decompression via a first rib resection and anterior scalenectomy. Stress urinary incontinence usually occurs as a result of urethral sphincter muscle weakness and/or an anatomical defect in the urethral support, leading to insufficient closure pressure in the urethral during physical activity. These defects usually present with an inability to tolerate feeds and abdominal distension within the first few days of life. It is best used for posterior horn, middle third, peripheral capsule, and bucket-handle tears. The long-term effect on range of motion is likewise dependent upon fracture pattern and displacement. Long-term clinical experience with fresh osteochondral allografts for articular knee defects in high demand patients. Drawing the portal sites and palpable landmarks as well as the ulnar nerve is useful before insufflation of the joint. The anteromedial portal is positioned 1 cm medial to the medial border of the superior aspect of the patellar tendon.
The severity of the infection depends on the nature of the disease and on patient-related factors. It is necessary to look in the posterior recesses and underneath the menisci for chondral pieces. On loading, these pins act as cantilevers and produce eccentric loading characteristics. The adductors usually are strained in an eccentric contraction, often one that occurs at the myotendinous junction, but the strain also can occur in the tendon itself or its bony insertion. Adhesions within the bursa can be cleared, providing excellent visualization of the iliopsoas tendon. This reamer need only be advanced enough to open the cortex and provide access to medullary contents. The adductor magnus inserts on the adductor tubercle, leading to a varus deformity of the distal segment. Although the Trendelenburg and Perthes tests can be useful, the inherent inaccuracies of applying the tourniquet or elastic bandages and the presence of other more direct objective testing modalities have led to a decrease in their use. Many different device systems exist with slight variations of technique and implant design. Once the incision has healed, a progresive strengthening and stretching routine is initiated, with an emphasis on core stabilization. The three sets are intertwined counterclockwise in the same fashion, resulting in a cord of nine total sutures. Posteromedial intra-articular tibial fragments need buttress plates to prevent varus collapse even with newer locking plate technology. Current recommendations for rotator interval closure include greater then 1 sulcus sign, laxity with a posterior component, and a collision athlete. Individuals suspected of having a concomitant sports hernia are referred to a general surgeon for definitive management. The length of this limb depends on the amount of posterior column that must be accessed. For horizontal cleavage tears, one or both "leaves" can be resected, depending on surgeon preference. A vaginal discharge from these conditions or from uterine abnormalities may give rise to pruritus vulvae, and there may be visible erythema, eczematous changes, excoriation and scratch marks. The surgical plan should include addressing concomitant pathology concurrently, as appropriate. Arthroscopic versus open treatment of Bankart lesion of the shoulder: a prospective randomized study. Because large quantities of fluid are produced, pass through the gastrointestinal tract daily and are reabsorbed in the small bowel and colon, large losses through vomiting and any intraluminal sequestration of fluid rapidly produce symptoms of dehydration. The supraspinatus tendon has a watershed area of hypovascularity located 1 cm medial to the insertion of the rotator cuff. For lateral transplants, the surgeon should strongly consider commercially available graft preparation instrumentation. Antegrade transarticular drilling is straightforward and creates channels that heal with fibrocartilage on the joint surface. Bowel Obstruction Transvaginal ultrasound is an excellent way to visualize the uterus and adnexae. In patients with any retropatellar tendon contracture, this tendon also is released to free up the extensor mechanism. The effect of manipulation under general anesthesia: structure and glycosaminoglycan content of the joint capsule. The bars can be configured in many ways, all of which provide temporary stabilization across the knee joint. Fracture of the penis (rupture of the cavernosal tunica albuginea) can occur when the erect penis slips out of the vagina and is compressed against the symphysis pubis. This way the bone plugs on the graft can be oversized, in the unlikely event that the new tunnel and old tunnel substantially overlap and create a bony defect that is considerably larger than the standard tunnel size.
The use of radiography, magnetic resonance, and ultrasound in the diagnosis of hip, pelvis, and groin injuries. The typical steps-using the opening drill, placing the guidewire, and reaming-are all completed through the elongated cannula. Ten to 15 mL of water-soluble contrast is then injected into the urethra and the outlet view of the pelvis is repeated. A percutaneous technique for anchor insertion can be employed using needle localization and a trocar and anchor guide through a posteroinferior stab incision. In a more recent study, however, the incidence of degenerative changes was significantly higher at 6- to 26-year follow-up in first-time dislocators treated nonoperatively. In contrast to most patients with an uncomplicated pyelonephritis, those who present with a perinephric abscess have usually been symptomatic for at least a week. Central anteromedial portal Anterolateral portal Accessory anteromedial portal Contraindications We have not found any contraindication to this procedure in the skeletally mature patient. Despite advances in diagnostic technology, the cornerstone in the evaluation of the urology patient remains a thorough medical history and physical examination. A branch of the superior gluteal artery feeds the largest nutrient foramina on the external surface in the center of the iliac wing, just anterior to the anterior gluteal line. The natural history of articular cartilage injuries currently is poorly understood. However, an imperfect reduction of the anterior pelvic ring and subsequent rigid stabilization may actually impair reduction of the more important posterior ring. Subjective and objective findings of instability should be present to support consideration of revision surgery. All patients had capitellar remodeling on follow-up radiographs, and approximately 42% had associated radial head enlargement. Emesis is usually non-bilious but can be bilious if the level of obstruction is just distal to the ampulla of Vater. This can be done through the anterosuperolateral portal with a Viper or Scorpion suture passer (Arthrex) loaded with a free no. Mesenteric panniculitis (sclerosing mesenteritis) is an idiopathic disease of inflammation and fibrosis that affects the mesenteric fat. Frozen shoulder: a prospective clinical study with an evaluation of the three treatment regimens. The posteromedial approach decompresses the superficial and deep posterior compartments. A three-point distraction device that applies longitudinal and vertical traction allows distraction of the humerus. Placing the second wire at the entry site and measuring what is not overlapping with the inserted wire provides nail length. Chondrocytes that produce the extracellular matrix are of mesenchymal stem cell origin. The posterior portion of the medial compartment is usually best visualized with the leg at 30 degrees, with a valgus stress applied to the knee. The cysts are typically located in the A varicocele is a dilatation of the veins of the pampiniform plexus within the spermatic cord. There could be a total of 85% to 90% reduction in pressure by just taking off the cast. Different patient showing the penetration of the medial side with the guidewires to allow plate placement. Anteriorly, a capsular incision is made along both the acetabular rim and the base of the femoral neck. Patients with a competent ileocaecal valve effectively have a closed-loop large bowel obstruction leading to severe pain and progressive abdominal distension with localized peritonitis over the colonic segment involved. Hemostasis should be meticulous, and proper drainage of hematoma implemented as needed. Several factors, including tear size, tendon and bone quality, and preoperative motion, should be considered in this decision. A skin incision is made at the entry site, large enough to faciliate entry of a 5. This attachment can be used in the reconstruction if the length is adequate; if not, it can be sutured to the reconstruction.
With a uterine cause of pain, such as tension on the round ligament, the point of maximal tenderness will shift to the left along with the uterus. Once healed, only showering, without any other pin cleaning procedures, is necessary. The skin incision and the dissection are performed as described for the tibial inlay technique. Resurfacing with osteoarticular allografts or autografts is not generally favored because the bony bed is dead. Right Heart Failure Chronic right heart failure may cause hepatic congestion resulting in ascites, hepatomegaly and even splenomegaly. Tagging sutures can be placed during the approach to allow for quick and effective soft tissue coverage over the repair. Indications for labrectomy include relief of pain with intraarticular injection of anesthesia, no pain relief with physical therapy or nonsteriodal anti-inflammatory drugs, missed time due to delayed diagnosis, and symptoms for longer than 4 weeks. Reliability of classification systems for intertrochanteric fractures of the proximal femur in experienced orthopaedic surgeons. Indomethacin is generally considered safe and effective, although a randomized trial has questioned its utility in prevention. We prefer 2 weeks with the knee in extension, 2 weeks of knee flexion from 0 to 60 degrees, and 2 weeks of full knee flexion in a hinged knee brace. Small impaction injuries associated with anterior dislocation also may be treated nonoperatively in many cases. Prostatitis Prostatitis is inflammation of the prostate gland that clinically presents as several syndromes with a range of clinical symptoms and investigative findings (Table 39. Therefore, minimally invasive techniques with the least possible soft tissue stripping and soft tissue irritation should be used. The anterior and posterior columns form an inverted Y and are attached to the sacrum via the sacral buttress. Patients who develop a ureterovaginal fistula following pelvic surgery often experience fever, flank pain and gastrointestinal symptoms post-operatively secondary to urinary extravasation. Transfer is indicated in these situations; otherwise, nonoperative treatment may be the only option. The lesion is fixed in place with an absorbable pin (three were used to fix this lesion). An understanding of the aetiology and anatomy is fundamental to the correct management. Bennett2 also found encouraging results in his prospective cohort with 2- to 4-year follow-up. In the elderly population, optimization of medical conditions is advisable, including evaluation of hydration and cardiac and pulmonary function, and management of chronic medical conditions. These include avoidance or correction of deformity, maintenance of stability, and pain-free function. The anterosuperior labrum is highly variable and in this case presents as a sublabral hole (arrow). These are often encountered as incidental findings during appendicectomy for presumed acute appendicitis. As with the iliopsoas, this often is a dynamic process, better demonstrated by the patient than produced by passive examination. These do not permit abdominal access, they require skill and familiarity, and they conceal the abdomen. Compensatory mechanisms may be insufficient in the elderly and in patients with cardiovascular and other medical comorbidities, in whom deterioration occurs rapidly. A positive result is defined as pain with resisted forward flexion and pronation; pain is diminished or relieved with supination. Next, a blunt trocar is introduced into the joint, followed by the 4-mm, 30-degree arthroscope.
The superior gluteal nerve, formed from the posterior divisions of L4, L5, and S1, passes posterior and lateral to the obturator internus and piriformis muscles, then between the gluteus medius and minimus muscles approximately 4 cm proximal to the hip joint. By manipulating the bone and its overlying cartilage, the articular surface is reduced to the femoral head with its intact cartilage. Although the subscapularis is the largest of the rotator cuff muscles, historically it has received little attention. The sutures are then easily identified and grasped, unloading from the knot pusher, which is withdrawn without difficulty. The distal clavicle is found in two orientations, either subacromial or subcoracoid, behind the intact conjoined tendon. In women, the cervix uteri can be felt projecting through the anterior rectal wall. The pain is constant and exacerbated by movement of the abdominal wall, such as in walking and coughing. If prone positioning is a concern, such as in patients with a high body mass index or compromised lung volume, the case is probably best done in the lateral decubitus position. For anteromedial tibial tubercle transfer, the cut proceeds obliquely from medial to lateral, tapering toward the anterior crest distally. Once the soft tissues have healed, conversion to definitive internal fixation can be safely accomplished. Spear guide is carefully positioned on the glenoid rim and held firmly in place during drilling and anchor insertion. Examine the area of reported pain last to avoid putting the patient in distress for the majority of the examination. Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated either with intramedullary nailing with reaming or with a plate: a comparative study. The patient must be closely monitored for the systemic effects of compartment syndrome. Positioning Iliotibial Band Various techniques have been described for correcting snapping of the iliotibial band. Making clear full-thickness flaps during the approach and using tagging sutures allows for secure coverage of the grafts and clavicle. Terminal stretching is continued for the next several months postoperatively, especially posterior capsule stretches. Screw Placement Screw fixation is performed as described above for percutaneous stabilization. Toe-touch weight bearing is permitted for 6 to 12 weeks depending on radiographic and clinical healing response. Clinical evidence of spontaneous healing of partial-thickness tears also appears limited. Urine is normally a pale yellow colour as a result of the pigment urochrome, but it can become discoloured from food substances, medications, products of metabolism, blood and infection. We prefer to decrease dead space, and therefore areas for hematoma to collect, with a layered closure, when possible, between the fascia lata and the skin. Once pain is alleviated, the postinjection increase in passive and active range of motion is recorded. The C-clamp can also be used to maintain reduction before plating if conventional clamps cannot hold the reduction. Ninety degrees of flexion is the optimal position for visualizing the posterolateral compartment of the knee. The anterior labroligamentous periosteal sleeve avulsion lesion: a cause of anterior instability of the shoulder. A resisted rotator cuff and periscapular strengthening program is initiated the third week postoperatively.